Long Island (LI) is one of the more socially and culturally diverse regions in NYS and in the US with population. LI residents are White (79%), Black (10.9%), Asian (7.4%) and other non-white races. Latinos make up 18.9% of the LI population.
LINCATS will address health equity through unique community/researcher collaborations that drive innovations to clinical and translational science with a hand on the pulse of underrepresented groups across Long Island. At the forefront of our efforts are addressing the health disparities present in our communities. Racial and socioeconomic health inequities manifest across many health outcomes.
Disparities in Cancer
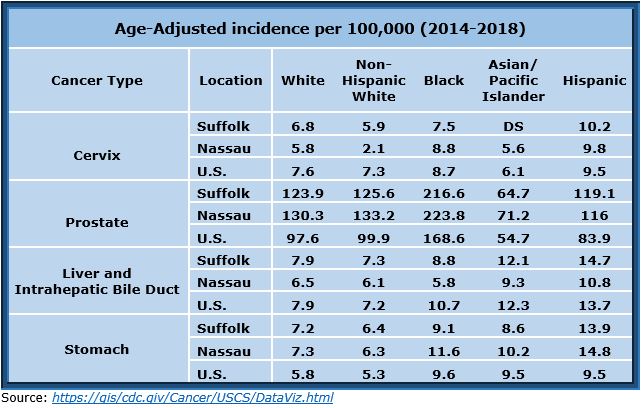
The second leading cause of death on Long Island is cancer. This rate is 15% higher than the US average, 7% higher than NY State, and further reflects the racial disparity trends across the U.S. On Long Island, there are disparities in cancer incidence compared to Non-Hispanic Whites with higher incidences for:
- Cervical Cancer among Hispanic people
- Prostate Cancer among Black people
- Liver and Intrahepatic Bile Duct Cancer among people of Asian/Pacific Islanders and Hispanic racial ethnicity
- Stomach Cancer among people of Black, Asian/Pacific Islander and Hispanic racial ethnicity
Disparities in COVID-19
COVID-19 data from 2020-2022 show a correlation between median household income and risk of COVID-19 infection. To help explain these differences, utilizing COVID-19 exposure maps, we overlaid regions (in Gray textured areas) from federally defined historically disadvantaged populations. These areas are home to >290,000 African Americans, >470,000 reporting Hispanic ethnicity, and >16,000 American Indians, representing over 1/3 of our catchment area’s populations. COVID-19 infection risk (darker red areas) was higher in regions with disadvantaged populations.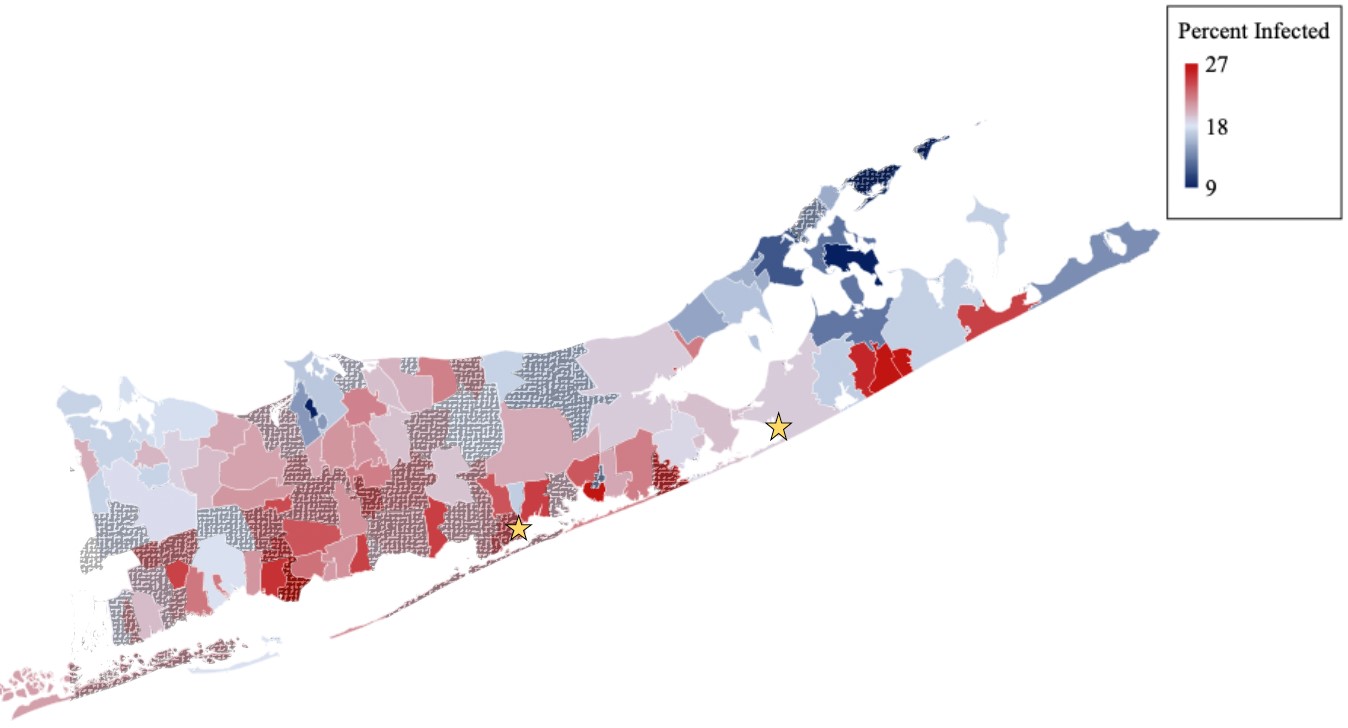
Prevalence of COVID-19 cases per 100 residents from June 2020-February 2022. Textured areas show a correlation between median household income and risk of COVID-19 infection. Stars designate Shinnecock and Unkechaug nations.
In 2020, at the start of the first wave of the COVID-19 pandemic, SBU Biomedical Informatics (BMI) launched a software informational BOT directly responding to the communities’ inquiries and priorities concerning the disease. In its first year, the BOT served over 10,000 individuals. The BOT disseminated information about the rapidly changing guidelines for COVID-19 to the community. BMI built an interdisciplinary team that drove rapid success. Building on this framework, and through community engagement, the public-facing BOT addressed community public health concerns within days. The focus on healthcare disparities led to the deployment of a Spanish language BOT, providing enhanced communication to mitigate the effects of social isolation of the pandemic on URGs and to address health care misinformation in these communities
LINCATS will continue to integrate community level needs and concerns; data from our system collaborators in the Community Advisory Board; and large data sets from the UDS Mapper, Census Bureau or in our Research Data Warehouse to develop generalizable contributions to clinical and translation science in an effort towards greater health equity.